Contrary to what a lot of people think. Radiology is not a big "Where's Waldo" game. It's about knowing the pattern of normal and disease, knowing what's clinically significant and what's just a normal variant, knowing what other findings go with the one that you see, knowing what findings go with the lab tests and physical exam findings that clinicians report. It turns out the describing what you see and communicating your idea of what the findings may represent is tougher than it seems.
In radiology, there is the concept of an "Aunt Minnie" (as evidenced by the popular radiology website). It refers to knowing what an abnormality is because you've seen it before. In other words, it's hard to describe what you see, but if you've seen it before, you know it can't be anything else. The trouble is that description is a large part of radiology. I should be able to convey what I see to a clinician to such a degree of accuracy that the clinician should be able to picture what I see without having the images in front of them (because this is, in fact, usually the case). This, I've found out is incredibly hard. I see what I want to describe pretty quickly, but it takes me several tries to be happy with how I've described it (then the attending changes it anyway).
In addition to finding the right words to describe something, there's conveying the clinical significance of what I see. There are hundreds of minor abnormalities or normal variants in an imaging study and we're obliged to describe them (so that someone else doesn't think that they represent a serious abnormality or doesn't spend thousands of dollars to further investigate it), but we must describe them in a manner that tells the clinician not to worry about it. For example, using words like "tiny" or "of questionable clinical significance" or "a normal variant" tells the clinician that we're not worried about it. Sometimes, it isn't that easy. Today, I saw a bone lesion that I thought was a small fragment from a vertebral fracture, but the attending I was working with was not worried about it. My dilemma was how to describe a fragment of bone near the spine of someone who is having neck pain and convey that it's not a big deal and is likely not what is causing the patients pain. It took me about six tries before I settled on something I was happy with.
The nice thing about these wording difficulties is that once I figure out something I'm happy with, I can use it for every other similar case. This is a major part of what my first year is all about.
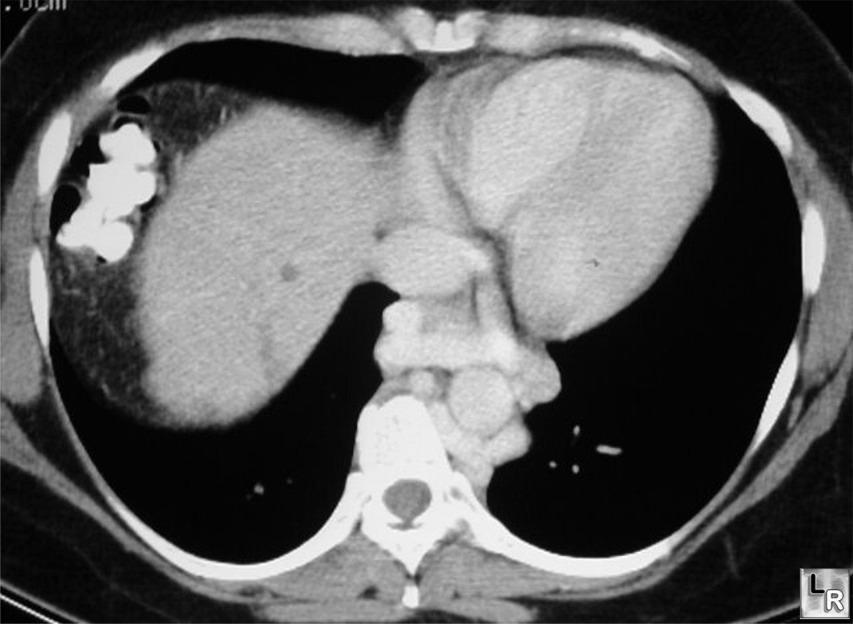 |
| I knew these were varices, but I got reprimanded by the attending for just saying "esophageal varices are present." It turns out I should have said "paraesophageal serpigenous enhancing tubular structures likely represent varices." (image from LearningRadiology.com) |
Don't you just end every radiology dictation with "Needs clinical correlation" anyway? :-)
ReplyDeleteBut seriously, sounds like you're having a very similar start to your radiology residency as I am with my neurology residency. There's both the art of diagnosis, as well as the art of conveying this information to others. Although I have primary patients, we are largely a consultative discipline, and there are real consequences to how we convey information to others. I'm learning a lot working with the neuro-radiologists and doing my own reads, but it is difficult. And as clinicians as a whole move away from physical exam and rely on radiology to tell us the answers, more of that burden is going to fall with you. Sooooo, good luck with that, my friend.
Oh, I've been trying my hardest to avoid saying "needs clinical correlation." I've also tried to avoid things like "These findings may be due to inflammation, infection or malignancy." :)
ReplyDelete